Overview
Dr. Jeff Chambers treated a calcified left anterior descending (LAD) using orbital atherectomy.


Dr. Jeff Chambers treated a calcified left anterior descending (LAD) using orbital atherectomy.
A 65 year old male presented with chest pain and had a stress echo where he exercised for 06:56 seconds, electrocardiogram (EKG) revealed mild ST depression less than 1 mm at peak stress, but stress echo showed a moderate-sized area of apical ischemia.
Past medical history includes obesity, borderline diabetes, hyperlipidemia, sleep apnea, a history of retinal artery occlusion and history of present illness (HPI). Patient was referred for coronary angiography.
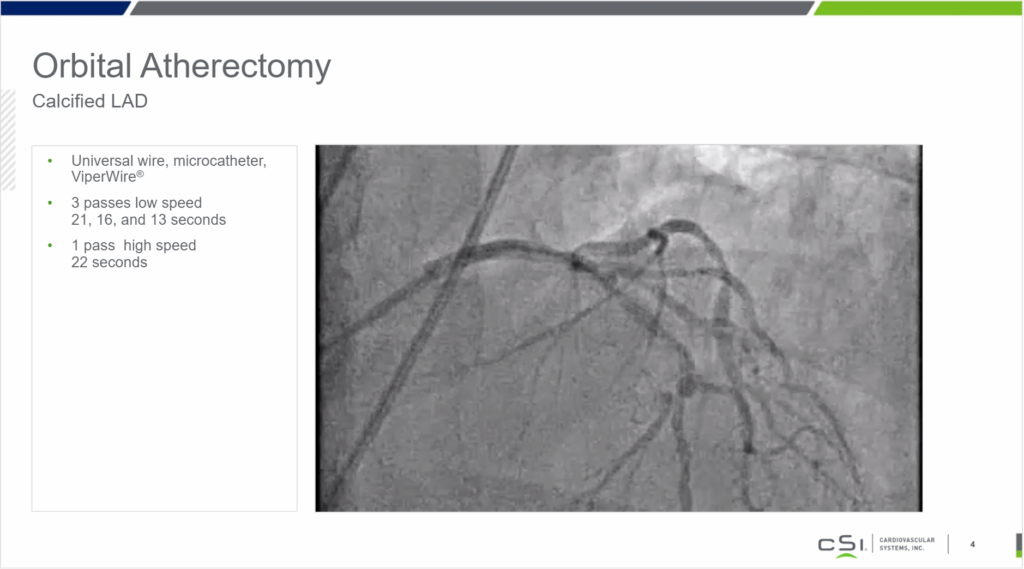
The patient’s baseline angiogram showed a severely calcified proximal LAD and the proximal LAD had a complex lesion just after the first diagonal, which was about 80 to 85 percent.
Then the LAD was calcified in the mid vessel, another complex lesion at the site of a second diagonal, which again appeared to be about 80 to 85 percent. The other artery showed moderate disease with 65 percent lesions in the circumflex and OM1 and moderate disease in the right coronary artery, with 60 percent distal right coronary artery, 50 percent PDA and 50 percent PLA. This was assessed with fractional flow reserve (FFR), it was decided to proceed with intervention.
Orbital atherectomy was selected to treat the lesions. A universal wire was preloaded in a micro catheter, then exchanged for the ViperWire Advance(R). The proximal LAD was treated with three passes on low speed and one on high speed.
A 2.5 x 12 NC balloon was expanded in the mid LAD to 10 atms yielding good balloon expansion. This was followed by a 3.0 x 12 balloon to 12 atms in the proximal LAD, also with good expansion. A 2.75 x 24 drug eluting stent was placed in the mid LAD across the second diagonal, deployed this at 12 atms. A 3.0 x 24 drug eluting stent was placed in the proximal LAD, overlapping with the mid LAD stent and extended almost back to the ostium, deployed at 12 atms.
The lesion was then post dilated with a 3.0 x 20 NC balloon in the proximal vessel and a 2.75 x 20 balloon in the mid LAD. Both were treated at 16 atms. Very good angiographic results confirmed the success of this procedure.
Given the severe calcium, stent expansion would not have been able to have been achieved without orbital atherectomy on this case.
Pre-Procedure
Post-Procedure
Post-Procedure
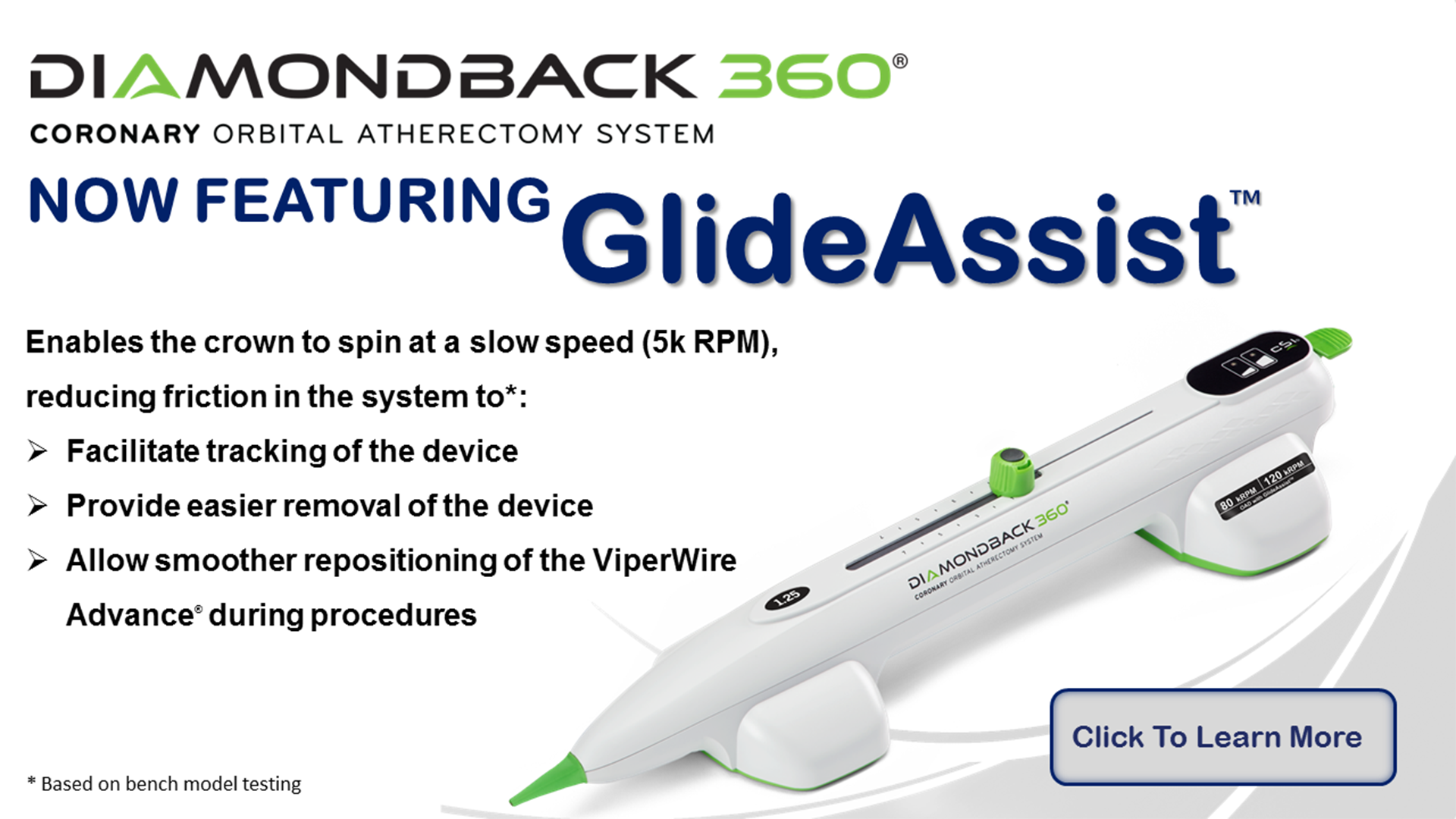
Indications Statement: The Diamondback 360® Coronary Orbital Atherectomy System (OAS) is a percutaneous orbital atherectomy system indicated to facilitate stent delivery in patients with coronary artery disease (CAD) who are acceptable candidates for PTCA or stenting due to de novo, severely calcified coronary artery lesions.
Contraindications: The OAS is contraindicated when the ViperWire Advance® Coronary Guide Wire cannot pass across the coronary lesion or the target lesion is within a bypass graft or stent. The OAS is contraindicated when the patient is not an appropriate candidate for bypass surgery, angioplasty, or atherectomy therapy, or has angiographic evidence of thrombus, or has only one open vessel, or has angiographic evidence of significant dissection at the treatment site and for women who are pregnant or children.
Warnings/Precautions: Performing treatment in excessively tortuous vessels or bifurcations may result in vessel damage; The OAS was only evaluated in severely calcified lesions, A temporary pacing lead may be necessary when treating lesions in the right coronary and circumflex arteries; On-site surgical back-up should be included as a clinical consideration; Use in patients with an ejection fraction (EF) of less than 25% has not been evaluated.
See the instructions for use before performing Diamondback 360 Coronary Orbital Atherectomy System procedures for detailed information regarding the procedure, indications, contraindications, warnings, precautions, and potential adverse events.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
Indications Statement: The Diamondback 360® Coronary Orbital Atherectomy System (OAS) is a percutaneous orbital atherectomy system indicated to facilitate stent delivery in patients with coronary artery disease (CAD) who are acceptable candidates for PTCA or stenting due to de novo, severely calcified coronary artery lesions.
Contraindications: The OAS is contraindicated when the ViperWire Advance® Coronary Guide Wire cannot pass across the coronary lesion or the target lesion is within a bypass graft or stent. The OAS is contraindicated when the patient is not an appropriate candidate for bypass surgery, angioplasty, or atherectomy therapy, or has angiographic evidence of thrombus, or has only one open vessel, or has angiographic evidence of significant dissection at the treatment site and for women who are pregnant or children.
Warnings/Precautions: Performing treatment in excessively tortuous vessels or bifurcations may result in vessel damage; The OAS was only evaluated in severely calcified lesions, A temporary pacing lead may be necessary when treating lesions in the right coronary and circumflex arteries; On-site surgical back-up should be included as a clinical consideration; Use in patients with an ejection fraction (EF) of less than 25% has not been evaluated.
See the instructions for use before performing Diamondback 360 Coronary Orbital Atherectomy System procedures for detailed information regarding the procedure, indications, contraindications, warnings, precautions, and potential adverse events.
Caution: Federal law (USA) restricts this device to sale by or on the order of a physician.
Results may vary.
Suggestions on case studies offered by the physician are based on their experience using the Diamondback® Orbital Atherectomy System and are their opinion. Medical decisions for your patients are to be based upon their condition and your medical judgment. CSI does not recommend or endorse any particular course of treatment or medical choice. Before using any medical device, including those demonstrated or referenced in this case study, review all relevant Instructions for Use, with particular attention to the indications, contraindications, warnings and precautions, and steps for use of the device.
At CSI, weare a culture of innovation.
We observe carefully, listen closely and collaborate extensively,
seeking opportunities to help interventionalists do their jobs more easily and more effectively –
all with the goal of improving patient care.
